Najeeb Ahmed, M.D.
Ripudeep Rai, M.D.
M. Atiq Khalid, M.D., F.A.C.C.
Department of Internal Medicine
Wright State University School of Medicine
Lipomatous Hypertrophy of the Interatrial Septum (LHAS) is an unusual condition caused by the excessive deposition of adipose tissue in the interatrial septum, usually a benign condition and most often detected as an incidental finding on echocardiography. The classic finding is a homogenous, bi-lobed configuration of the interatrial septum with sparing of the fossa ovalis. This infiltration can also involve the septal tissue and has been associated with various atrial arrhythmias, including multifocal atrial tachycardia, multiple atrial premature contractions, atrial fibrillation and rarely even sudden death (1).
LHAS is a benign condition exclusively found in elderly patients in the seventh-eighth decade of life, rarely seen in younger age group. We report an unusual case of LHAS found incidentally in an asymptomatic young patient. A 35 year white female was admitted to hospital with a swollen right arm, fever and chills of two days duration. One week prior to this admission, she was admitted at an outside facility for atypical chest pain and underwent a stress test, which was negative for ischemia. She had a peripherally inserted central catheter (PICC) placed in the right arm during that admission and removed upon discharge from the hospital.
Her physical exam on admission showed a red, swollen and tender right upper extremity from the axilla to the elbow. The remainder of the physical exam was unremarkable. She underwent an ultrasound of her right upper extremity, which showed a deep venous thrombus (DVT) in the subclavian and axillary vein. Her blood cultures grew Staphylococcus aureus. She was referred for a transesophageal echocardiogram (TEE) to rule out endocarditis.
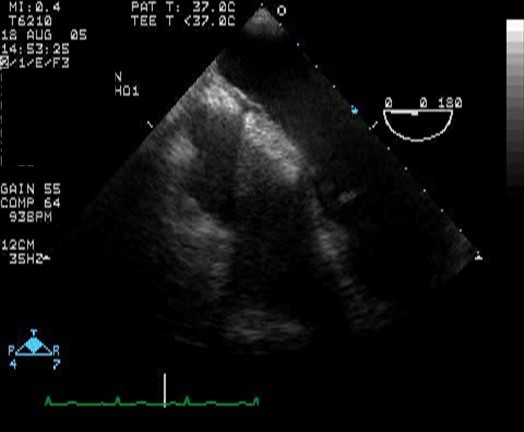
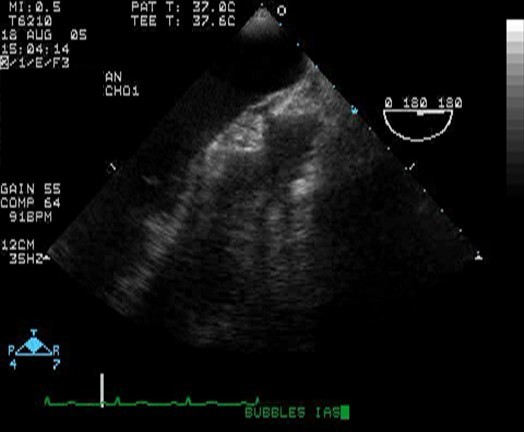
TEE incidentally revealed a bi-lobed echogenic hypertrophy of the interatrial septum, sparing the foramen ovale (Fig 1, 2) and no vegetations were seen on the valves.
Lipomatous hypertrophy of the heart is a benign rare condition characterized by large fatty tissue deposits in the interatrial septum, usually extending to the atrial wall and rarely to the interventricular septum. This condition is more common than true cardiac lipomas, occurring almost exclusively in elderly, obese patients and is usually asymptomatic.
Available data indicate that this condition is more likely to be seen in seventh to eighth decade of life, more commonly in women and with age-associated increases of epicardial fat. It is rarely seen in younger age group which mandate more extensive investigation to rule out true neoplasm. It is characterized histologically by the presence of granular or vacuolated fetal adipocytes and non-encapsulated, non-neoplastic mature fat cells. The absence of encapsulated fat cells and the presence of fetal fat cells distinguish it from lipoma (2, 3).
LHAS abnormality was first described by Prior in 1964 (4). It is usually benign and asymptomatic but a significant number of patients have been reported to have unexplained arrhythmias such as atrial fibrillation, atrioventricular (AV) block and sudden death (5). In most patients, it represents an incidental echocardiographic finding that requires no intervention.
Noninvasive modalities have led to identification of these masses, which may be mistaken for a tumor if massive. Computed tomography (CT), magnetic resonance imaging (MRI), transthoracic echocardiograms (TTE) and TEE allow simple non-invasive diagnostic imaging of the interatrial septum. TEE has the potential to provide enhanced resolution of the interatrial septum and may allow exact delineation of the structure?s extent when CT, MRI or TTE are not adequate (6).
TEE diagnosis of LHAS is based on the classic morphology of the thickened, echogenic bi-lobed septal mass (7). A variety of other cardiac lesions such as lipomas, liposarcomas, metastatic tumors, myxomas and amyloidosis can also present as a septal tumor mass. However LHAS, always spares the foramen ovale. Endomyocardial biopsy can be performed for further evaluation.
Surgical excision of the LHAS is reserved for patients who have superior vena cava (SVC) obstruction or an intractable rhythm disturbance (8, 9).
Pathologically it is hypertrophy of preexisting epicardial fat. The LHAS may extend into the region of the AV node and characteristically, the proximal and the distal part of the interatrial septum are most markedly involved with sparing of the fossa ovalis , as was the case in our patient with LHAS.
In conclusion, LHAS is a rare, benign deposition of fatty tissue within the interatrial septum, often diagnosed incidentally and usually not requiring intervention. LHAS must be included in the differential diagnosis of any right atrial mass, or any fat-containing neoplasm. CT and TEE are the diagnostic tools of choice. Surgical correction must be considered in cases of severe rhythm disorders or great vessel obstruction.
Back to E-chocardiography Home Page.

The contents and links on this page were last verified on November 3, 2005.